Overview
Pantai Hospitals is one of Malaysia's largest private hospital groups, operating 5 major facilities with hundreds of facility management staff across housekeeping, maintenance, and operations teams. When I joined this engagement, the entire operations layer ran on paper work orders, radio calls, and disconnected spreadsheets — and the cost was measurable: 4.5-hour average maintenance response times, 61% of management time consumed by manual reporting, and no real-time visibility into what was happening across any facility at any given moment.
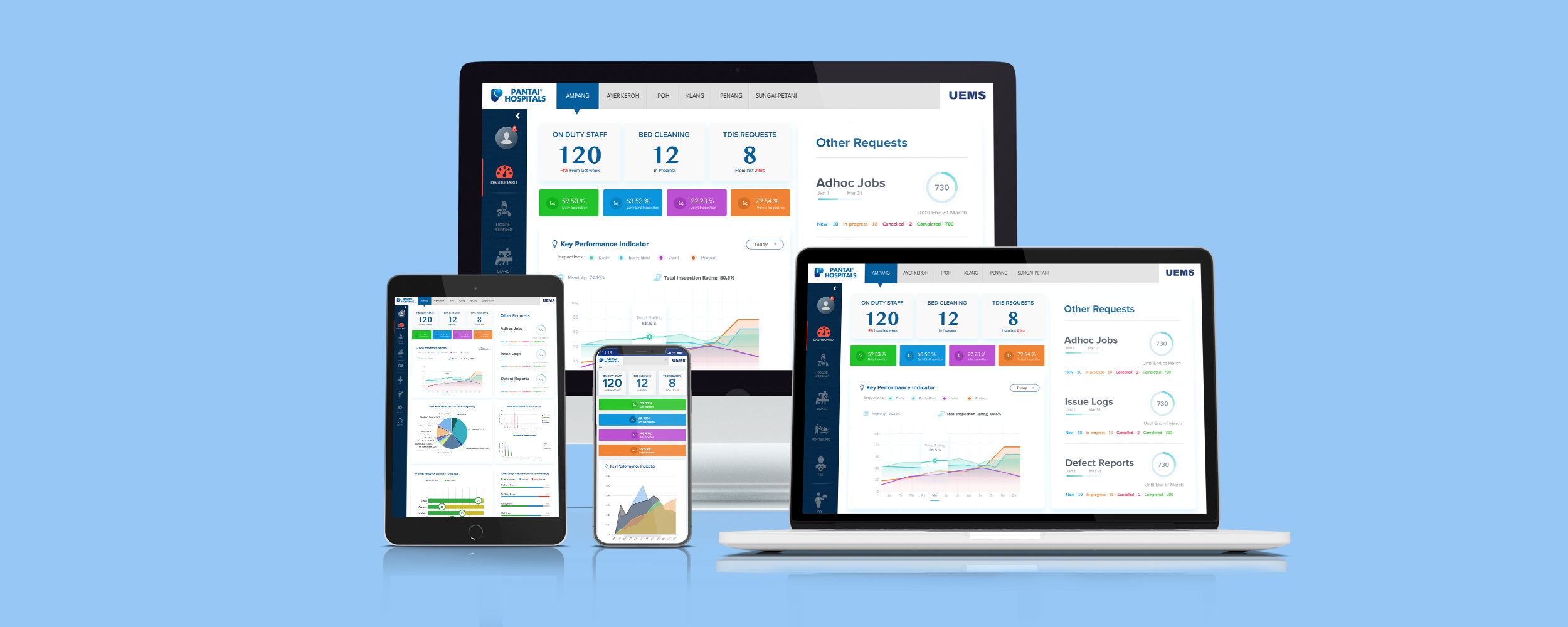
I was brought in as Lead Product Designer to design a role-based enterprise dashboard from the ground up — a single platform to replace every fragmented system, giving each user type — from the Facility Manager at their desk to the maintenance technician on the hospital floor — exactly the information they needed, in the right format, to act faster and with fewer errors.
This was the most complex design challenge I had taken on: three distinct user types with fundamentally different workflows, five physical locations, real-time data requirements, hospital-grade compliance constraints, and a six-month delivery timeline.
The problem
Before any design work began, I spent two weeks embedded alongside operations teams across two hospital sites. The problems were systemic, deeply normalised, and far more costly than management had realised.
Pantai Hospitals — facility management operations across 5 major sites in Malaysia
Facility managers spent most of their working day compiling reports from disconnected systems — leaving little capacity for actual operational decision-making.
Housekeeping supervisors coordinated teams entirely by radio. No visibility into task progress, no audit trail, no accountability system across a single shift.
Maintenance technicians collected paper work orders at physical stations across the building. No mobile access meant wasted movement and significantly delayed job acknowledgement.
Emergency maintenance requests passed through 3+ manual handoffs before reaching a technician. A critical patient-room request could take nearly half a working day to action.
Management had no real-time visibility. Resource allocation and shift planning decisions were made on data that was hours out of date.
Hygiene and safety compliance reporting required 3 days of manual data aggregation from paper records across all five sites — making compliance reactive rather than proactive.
Research & discovery
With six months to deliver a production platform, I front-loaded research heavily. The complexity — three user types, five locations, real-time systems, regulatory constraints — meant that assumptions made early would compound into expensive mistakes later. I treated the first six weeks as non-negotiable research time and structured it across five parallel workstreams.
What I did
I structured interviews around actual job tasks, not abstract questions. Each participant walked me through their last full shift — every tool they used, every point of friction, every workaround they had normalised. Across 35 staff members and 8 shift patterns, consistent failure patterns emerged within the first week.
I shadowed housekeeping supervisors, maintenance technicians, and facility managers through live shifts — day, evening, and handoff periods. This exposed what interviews couldn't: improvised workarounds staff had built into daily routines that no one had documented, and the communication breakdowns that occurred in real time during shift transitions.
I mapped response time patterns, bottleneck locations, and failure clusters across all five sites. This converted anecdotal frustrations into quantified problems — which became the specific KPIs the dashboard was designed to move, and the baseline against which post-launch impact was measured.
Not all metrics mattered equally. I facilitated a prioritisation session with the PM and hospital operations director to sequence which KPIs the dashboard needed to surface at launch versus which were phase-two additions — preventing scope overload while protecting the highest-impact requirements.
Before wireframes began, I ran a structured session with the three engineers covering HVAC integration constraints, hospital safety data compliance requirements, real-time notification architecture, and mobile-first technical requirements. These constraints were factored into design decisions from the start — not raised as blockers at handoff.
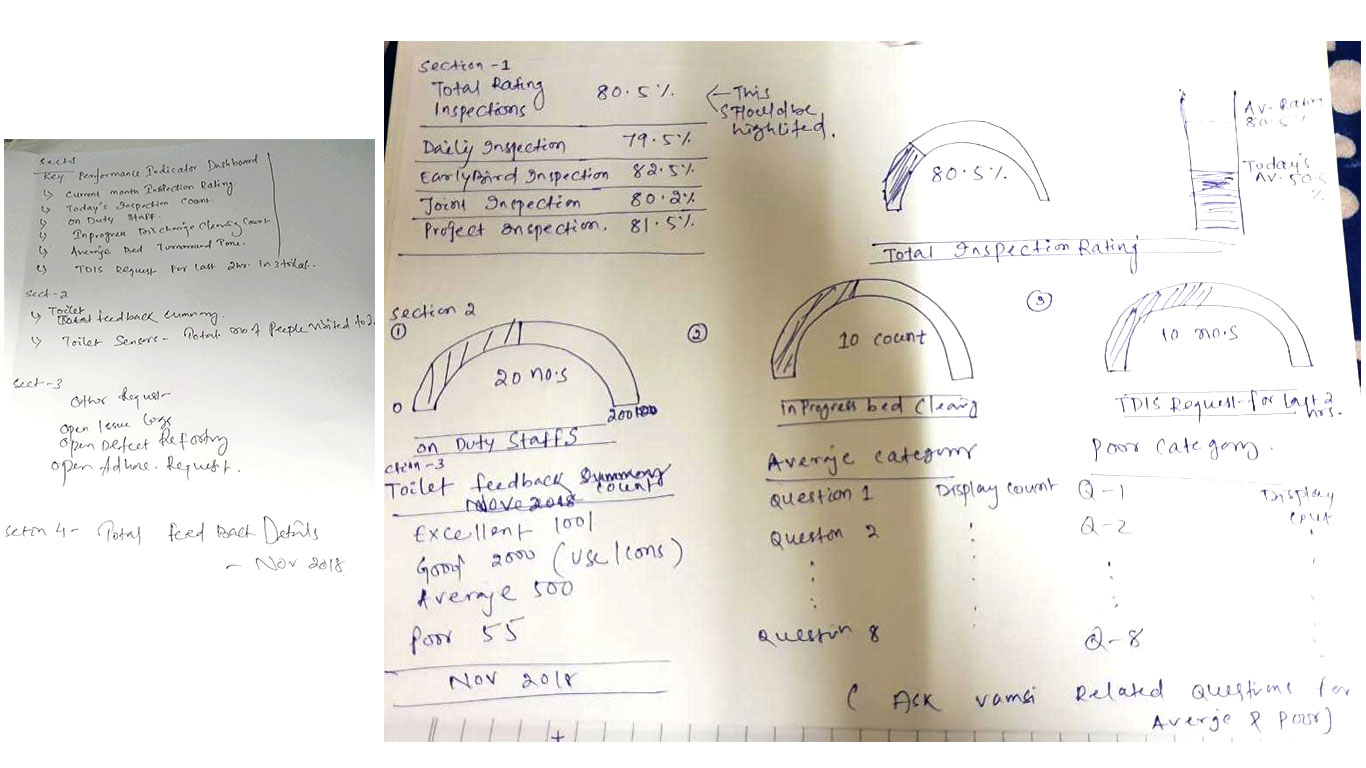
Research outputs: contextual sketches, workflow mapping, and early wireframes from synthesis sessions with the cross-functional team
Key insights
A single dashboard serving all three user types would have failed each of them. Every role needed fundamentally different information density, interaction patterns, and primary actions.
89% of operational tasks happened away from a desk. For technicians and supervisors, mobile wasn't an extension of the desktop experience — it was the entire experience.
The costliest operational errors occurred at shift changes when information wasn't reliably transferred. The design needed to make handoff communication structural and documented — not dependent on memory or verbal briefings.
Staff were trained to follow proven protocols. The UI had to feel immediately intuitive — learnable in a single shift — or adoption would fail regardless of technical capability.
User profiles
Research produced three distinct user profiles, each with fundamentally different goals, physical environments, and failure modes. Rather than one flexible interface, I designed three purpose-built views sharing a unified design system — giving each role exactly what they needed without the cognitive overhead of a general-purpose tool.
Facility Manager
- Real-time operational visibility across sites
- KPI monitoring and compliance tracking
- Resource planning and budget reporting
- Instant escalation of critical issues
- No live view — all data hours out of date
- Manual report compilation consumed the working day
Housekeeping Supervisor
- Real-time team location and task status
- Assign and reassign tasks without radio calls
- Infection control standards tracking
- Supply and inventory visibility
- 43+ radio calls per shift — no digital audit trail
- Paper-based task assignment with no completion tracking
Maintenance Technician
- Receive and acknowledge jobs on mobile instantly
- Access technical documentation in the field
- Update job status in real-time
- Communicate with supervisor without radio
- Physical work order collection added 3+ miles of daily unnecessary travel
- No priority indication — critical jobs looked identical to routine ones
Design decisions
After presenting research findings to the PM and operations director, I mapped each problem to a specific design decision and secured alignment before moving into wireframes. Every decision below was traceable to a research finding. The guiding principle across all of them: reduce cognitive load in a high-stakes environment. Healthcare workers can't afford to interpret an interface — the right action has to be obvious.
Three purpose-built views, one unified design system
The temptation in enterprise design is to build one configurable system that serves everyone. The research made clear this would fail: a Facility Manager needs data density and multi-site overview; a Housekeeping Supervisor needs team coordination and task assignment; a Maintenance Technician needs a stripped-back mobile interface with a single primary action. I designed three distinct views — each optimised for its user's tasks, environment, and decision context — all sharing a single Figma component library with consistent tokens, patterns, and visual language. Unified system, differentiated experiences.

Facility Manager command centre — live KPI monitoring across all 5 sites, with critical issue escalation surfaced at the top of the hierarchy
Progressive disclosure to eliminate cognitive overload
In a high-pressure healthcare environment, information overload is as dangerous as information absence. I applied strict progressive disclosure throughout every view: each surface showed only what the user needed to act right now, with secondary detail accessible on demand. Critical issues — maintenance emergencies, infection control alerts — were elevated with a red-priority system that made them visually impossible to miss and semantically impossible to confuse with routine tasks. This priority distinction was the most-cited improvement in post-launch feedback from all three user groups.
Replaced paper work orders with a mobile-native job flow
The technician experience was designed mobile-first from the start — not adapted from a desktop layout. Jobs appeared as a prioritised list with clear urgency indicators, one-tap acknowledgement, inline technical documentation, and status updates that pushed instantly to the supervisor's view. Tap targets were set to 48px minimum throughout. The notification system was architected to surface critical requests within seconds of dispatch — eliminating the multi-handoff radio process that had averaged 2+ hours per critical job. This single flow change was the primary driver of the 65% reduction in maintenance response time.
Mid-fidelity wireframes: technician mobile job flow with priority indicators (left) and supervisor team coordination view with real-time task status (right)
Made shift handoffs structural, documented, and non-negotiable
Research identified shift handoffs as the single highest-risk moment in the operations cycle — where the most information loss occurred and the most consequential errors originated. I designed a dedicated handoff module that required outgoing supervisors to formally log outstanding tasks, in-progress jobs, and flagged issues before signing off their shift. The incoming supervisor received a structured written summary — replacing the verbal briefing — with one-tap acknowledgement that created a timestamped audit record. Post-launch, this was the feature supervisors described as the one they hadn't known they needed.
Turned 3-day manual reporting into a single export action
Hygiene and safety compliance reporting had required 3 days of manual aggregation from paper records across all five sites. I worked with the data analyst to map exactly which data points each compliance report required, then designed the platform to capture those data points passively — as a natural byproduct of normal system use, not as a separate logging task. The result: compliance reports became a one-click export. The 92% compliance rate post-launch reflected not just better visibility, but the fact that staff were completing tasks in the system that they had previously skipped because the paper trail was too cumbersome to maintain.
What failed — and what we changed
An enterprise project of this complexity doesn't travel in a straight line from brief to correct solution. Three significant design directions were tested, found to be wrong, and replaced. Documenting what didn't work matters as much as documenting what did.
One dashboard for all three roles — abandoned after the first usability test
My initial architectural proposal was a single platform with role-based toggles: a universal dashboard that surfaced different data depending on who was logged in. The engineering team favoured it for obvious reasons — one codebase, simpler onboarding. The first usability test with 6 real hospital staff participants broke the assumption completely. The Facility Manager needed multi-site data density and compliance trend analysis. The Housekeeping Supervisor needed real-time team status and fast task dispatch. The Maintenance Technician needed a stripped mobile interface with a single primary action at all times. None of them shared a workflow or decision context. A configurable interface would have produced a mediocre product for all three. I redesigned into three purpose-built views with a shared component library — the architecturally correct solution, even though it required significantly more design work.
Push notifications blocked on hospital networks — required full rearchitecture
The original real-time alert system for maintenance technicians relied on external push notification services. During the technical discovery session I ran with the engineering team before any wireframing began, we confirmed that hospital Wi-Fi across 3 of the 5 sites blocked external push services for network security compliance reasons. This invalidated the original technician alert flow entirely — a significant finding that would have become a launch-blocking problem if it had surfaced at handoff. Working with the backend engineer, we pivoted to a polling-based in-app notification system with a sub-60-second refresh cycle. Less architecturally elegant, but reliable across every hospital environment. The 65% response time reduction held regardless.
Smart routing algorithm removed from phase 1 after technical scoping
The original brief included an algorithm that would automatically assign incoming jobs to the nearest available technician based on real-time GPS location and skill-tag matching. After the data analyst scoped the backend requirements — continuous GPS polling, a skill taxonomy system, routing logic, and battery drain implications for staff devices — the PM and I agreed this was 6–8 weeks of engineering work that would delay the platform launch. We removed it from phase 1, replaced it with a supervised manual dispatch flow, and documented it as a full phase-2 brief. The manual dispatch still outperformed the radio system by an order of magnitude on every KPI we tracked.
Patient-room data and staff location tracking required review against Malaysia's Personal Data Protection Act. Several real-time features needed legal sign-off before design could proceed, adding 2 weeks to the discovery phase.
Hospital staff used personal devices ranging from current iPhones to low-spec Android handsets from 2019. Every mobile screen was tested at 320px minimum width and on a physical low-spec Android device before approval.
The platform had to ship within the financial year to unlock continued operational investment. Every scope trade-off was evaluated against this non-negotiable constraint throughout the engagement.
Hospital staff couldn't be removed from active duty for usability testing. Each session was scheduled around 30-minute shift breaks, requiring close coordination with the operations director across all 5 sites.
Process & cross-functional ownership
This was the most cross-functional project I have led as a designer. The six-month engagement required sustained coordination between design, engineering, hospital operations, and data teams — across five physical locations and multiple stakeholder tiers.
- Led all research planning, facilitation, and synthesis — 35 interviews, 80+ hours of on-site observation, and 6 months of operational data analysis — before any wireframing began.
- Presented a prioritised problem map and design strategy to senior operations director and PM prior to entering design. All design decisions were pre-aligned at this stage, preventing costly scope changes mid-build.
- Ran three rounds of moderated usability testing — prototype, mid-build, and pre-launch — with 6 hospital staff participants per round drawn from actual users across all three roles.
- Built the complete component library in Figma before screen design began: colour tokens, spacing system, role-specific priority indicators, mobile patterns, and accessibility annotations documented for developer handoff.
- Managed developer handoff with 3 engineers using annotated Figma specifications, a shared component inventory, and weekly design-development sync sessions throughout the build sprint — reducing implementation clarification requests significantly.
- Led a structured 90-day post-launch retrospective with the PM and operations director, quantifying the impact data above and identifying four design refinements that were shipped as a follow-up sprint.
Tools used
Results & impact
All outcomes were tracked over 90 days post-launch using platform analytics, operational data from hospital management systems, and a structured retrospective with the PM and operations director. Each result is attributed to the specific design decision that drove it.
- 65% reduction in maintenance response time (4.5hrs → 1.6hrs) — driven by the mobile-native technician job flow replacing the multi-handoff radio process. Instant push notifications eliminated the 2+ hour delay in emergency job assignment that had been the most costly bottleneck in the system.
- £1.8M estimated annual operational cost savings — calculated by the hospital operations director from reduced overtime costs, faster room turnover, and eliminated manual reporting labour across all 5 sites over a 12-month projection.
- 78% increase in technician productivity — technicians spent time completing jobs rather than collecting paper orders or waiting for radio confirmation. The combination of mobile access, clear priority indicators, and inline documentation removed the friction from every step of the job lifecycle.
- 92% preventive maintenance compliance rate — up from a baseline estimated below 60%. Compliance automation made adherence the path of least resistance: staff completed tasks in the system as a byproduct of normal use, rather than as a separate logging burden.
- 61% reduction in manager manual reporting time — facility managers recovered the majority of their working day. Live KPIs surfaced information that had previously required hours of spreadsheet compilation to produce.
- Shift handoff errors effectively eliminated — the structured handoff module replaced verbal briefings with documented, auditable summaries. Supervisors cited this as the most impactful individual feature in the post-launch survey.
Key takeaways
- Observational research surfaces what interviews miss. The 80+ hours on-site watching actual workflows produced the most valuable design inputs — particularly around shift handoff failures and normalised workarounds that no one would have described as problems in an interview.
- Role-specificity beats universal flexibility in enterprise design. The right call was three purpose-built views — each optimised for its user — which delivered faster staff adoption and lower training overhead than a single complex configurable interface would have.
- In healthcare, cognitive load reduction is a patient safety issue. Designing for low mental effort wasn't a UX preference here — it was a clinical requirement. Ambiguity in a high-pressure environment creates errors. Every design decision was evaluated against that standard.
- Compliance by design, not by enforcement. The 92% compliance rate didn't come from training harder — it came from making compliance the easiest path. When the system captured compliance data as a byproduct of normal use, adherence followed automatically.
- Quantify the problem before you design the solution. Going into this project with 6 months of operational data meant every design priority was backed by a number, every stakeholder conversation was grounded in evidence, and every post-launch metric had a clear baseline to compare against.
Reflection
The Pantai Hospitals project is the one I point to when someone asks what enterprise product design actually requires. It's not about making things look clean — it's about understanding a system deeply enough to redesign how it works, not just how it looks.
The most valuable skill I exercised wasn't visual design or interaction craft — it was research patience. Spending six weeks on-site before touching a wireframe felt slow in the moment. In retrospect, it was the decision that made every subsequent step faster and more confident. Every trade-off was informed. Every priority was grounded. The delivered product solved the actual problems, not the assumed ones.
I also learned something important about designing for high-stakes environments: the best interface earns trust immediately. For hospital staff trained to follow proven protocols and distrust unfamiliar systems, first-shift usability wasn't a nice-to-have — it was the product's entire credibility. That shaped every decision, from the priority colour system to error message tone to the way job types were visually differentiated on a 5-inch mobile screen.